
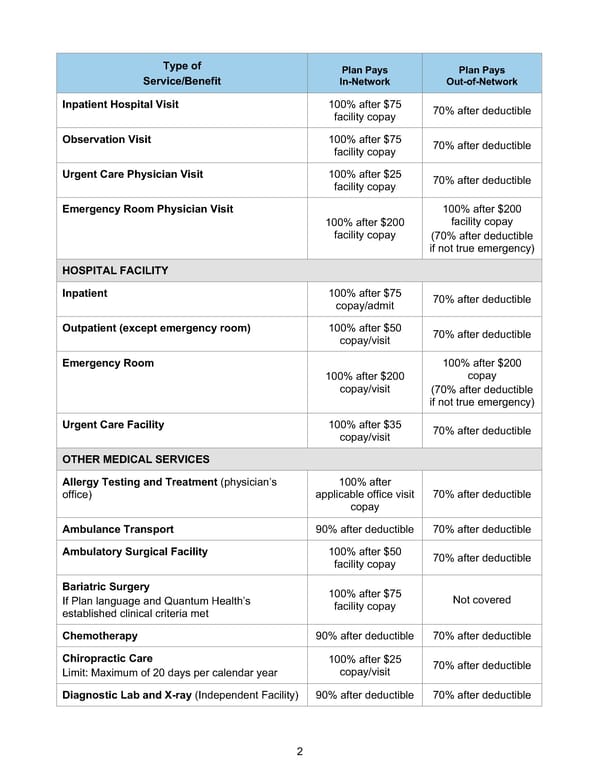
2 Type of Service/Benefit Plan Pays In-Network Plan Pays Out-of-Network Inpatient Hospital Visit 100% after $75 facility copay 70% after deductible Observation Visit 100% after $75 facility copay 70% after deductible Urgent Care Physician Visit 100% after $25 facility copay 70% after deductible Emergency Room Physician Visit 100% after $200 facility copay 100% after $200 facility copay (70% after deductible if not true emergency) HOSPITAL FACILITY Inpatient 100% after $75 copay/admit 70% after deductible Outpatient (except emergency room) 100% after $50 copay/visit 70% after deductible Emergency Room 100% after $200 copay/visit 100% after $200 copay (70% after deductible if not true emergency) Urgent Care Facility 100% after $35 copay/visit 70% after deductible OTHER MEDICAL SERVICES Allergy Testing and Treatment (physician’s office) 100% after applicable office visit copay 70% after deductible Ambulance Transport 90% after deductible 70% after deductible Ambulatory Surgical Facility 100% after $50 facility copay 70% after deductible Bariatric Surgery If Plan language and Quantum Health’s established clinical criteria met 100% after $75 facility copay Not covered Chemotherapy 90% after deductible 70% after deductible Chiropractic Care Limit: Maximum of 20 days per calendar year 100% after $25 copay/visit 70% after deductible Diagnostic Lab and X-ray (Independent Facility) 90% after deductible 70% after deductible
 BTF Summary Plan A/A+ Page 6 Page 8
BTF Summary Plan A/A+ Page 6 Page 8