
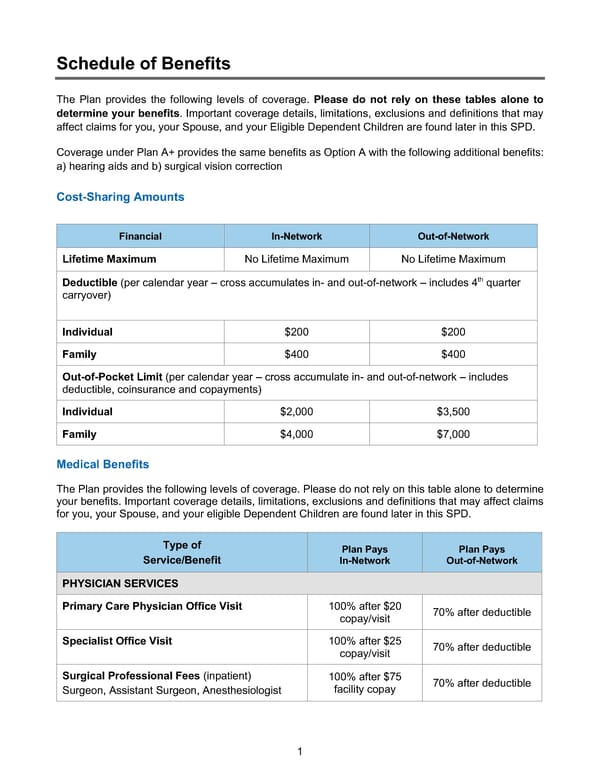
1 Schedule of Benefits The Plan provides the following levels of coverage. Please do not rely on these tables alone to determine your benefits. Important coverage details, limitations, exclusions and definitions that may affect claims for you, your Spouse, and your Eligible Dependent Children are found later in this SPD. Coverage under Plan A+ provides the same benefits as Option A with the following additional benefits: a) hearing aids and b) surgical vision correction Cost-Sharing Amounts Medical Benefits The Plan provides the following levels of coverage. Please do not rely on this table alone to determine your benefits. Important coverage details, limitations, exclusions and definitions that may affect claims for you, your Spouse, and your eligible Dependent Children are found later in this SPD. Type of Service/Benefit Plan Pays In-Network Plan Pays Out-of-Network PHYSICIAN SERVICES Primary Care Physician Office Visit 100% after $20 copay/visit 70% after deductible Specialist Office Visit 100% after $25 copay/visit 70% after deductible Surgical Professional Fees (inpatient) Surgeon, Assistant Surgeon, Anesthesiologist 100% after $75 facility copay 70% after deductible Financial In-Network Out-of-Network Lifetime Maximum No Lifetime Maximum No Lifetime Maximum Deductible (per calendar year – cross accumulates in- and out-of-network – includes 4th quarter carryover) Individual $200 $200 Family $400 $400 Out-of-Pocket Limit (per calendar year – cross accumulate in- and out-of-network – includes deductible, coinsurance and copayments) Individual $2,000 $3,500 Family $4,000 $7,000
 BTF Summary Plan A/A+ Page 5 Page 7
BTF Summary Plan A/A+ Page 5 Page 7