
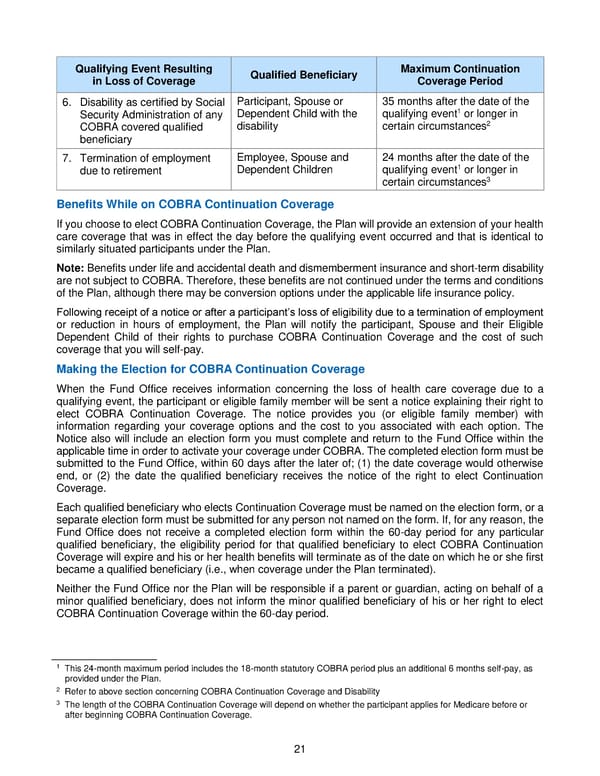
21 Qualifying Event Resulting i n Loss of Coverage Qualified Beneficiary Maximum Continuation Coverage Period 6. Disability as certified by Social Security Administration of any COBRA covered qualified beneficiary Participant, Spouse or Dependent Child with the disability 35 months after t he date of the qualifying event 1 or longer in certain circumstances 2 7. Termination of employment due to retirement Employee , Spouse and D ependent Children 24 months after t he date of the qualifying event 1 or longer in certain circumstances 3 Benefit s While on COBRA Continuation Coverage If you choose to elect COBRA Continuation Coverage, the Plan will provide an extension of your health care coverage that was in effect the day before the qualifying event occurred and that is identical to similarly situated participants under the Plan. No te: Benefits under life and accidental death and dismemberment insurance and short - term disability are not subject to COBRA. Therefore, these benefits are not continued under the terms and conditions of the Plan, although there may be conversion options un der the applicable life insurance policy. Following receipt of a notice or after a participant’s loss of eligibility due to a termination of employment or reduction in hours of employment, the Plan will notify the participant, Spouse and their Eligible Dep endent Child of their rights to purchase COBRA Continuation Coverage and the cost of such coverage that you will self - pay . Making the Election for COBRA Continuation Coverage When the Fund Office receives information concerning the loss of health care cove rage due to a qualifying event, the participant or eligible family member will be sent a notice explaining their right to elect COBRA Continuation Coverage. The notice provides you (or elig ible family member) with information regarding your coverage option s and the cost to you associated with each option. The Notice also will include an election form you must complete and return to the Fund Office within the applicable time in order to activate your coverage under COBRA. The completed election form must be submitted to the Fund Office, within 60 days after the later of; (1) the date coverage would otherwise end, or (2) the date the qualified beneficiary receives the notice of the right to elect Continuation Coverage. Each qualified beneficiary who elects Continuation Coverage must be named on the election form, or a separate election form must be submitted for any person not named on the form. If, for any reason, the Fund Office does not receive a completed election form within the 60 - day period for any pa rticular qualified beneficiary, the eligibility period for that qualified beneficiary to elect COBRA Continuation Coverage will expire and his or her health benefits will terminate as of the date on which he or she first became a qualified beneficiary (i.e ., when coverage under the Plan terminated) . Neither the Fund Office nor the Plan will be responsible if a parent or guardian, acting on behalf of a minor qualified beneficiary, does not inform the minor qualified beneficiary of his or her right to elect COBRA Continuation Cov erage within the 60 - day period. 1 This 24 - month maximum period includes the 18 - month statutory COBRA period plus an additional 6 months self - pay, as provided under the Pla n. 2 Refer to above section concerning COBRA Continuation Coverage and Disability 3 The length of the COBRA Continuation Coverage will depend on whether the participant applies for Medicare before or after beginning COBRA Continuation Coverage.
 2018 BTF Plan C Page 25 Page 27
2018 BTF Plan C Page 25 Page 27