
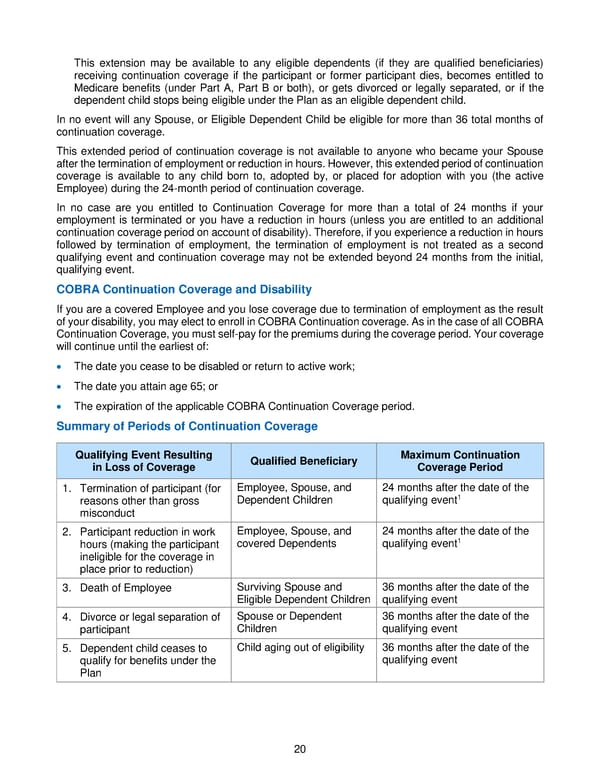
20 This extension may be available to any eligible dependents (if they are qualified beneficiaries) receiving continuation coverage if the participant or former participant dies, becomes entitled to Medicare benefits (under Part A, Part B or both), or gets divorced or legally separated, or if th e dependent child stops being eligible under the Plan as an eligible dependent child. In no event will any Spouse, or Eligible Dependent Child be eligible for more than 36 total months of continuation coverage. This extended period of continuation co verag e is not available to anyone who became your Spouse after the termination of employment or reduction in hours. However, this extended period of continuation coverage is available to any child born to, adopted by, or placed for adoption with you (the a ctive Employee) during the 24 - month period of cont inuation coverage. In no case are you entitled to Continuation Coverage for more than a total of 24 months if your employment is terminated or you have a reduction in hours (unless you are entitled to an ad ditional continuation coverage period on account of disability). Therefore, if you experience a reduction in hours followed by termination of employment, the termination of employment is not treated as a second qualifying event and continuation coverage ma y not be extended beyond 24 months from the initial, qualifying event. COBRA Continuation Coverage and Disability If you are a covered Employee and you lose coverage due to termination of employment as the result of your disability, you may elect to enrol l in COBRA Continuation coverage. As in the case of all COBRA Continuation Coverage, you must self - pay for the premiums during the coverage period. Your coverage will continue until the earliest of: • The date you cease to be disabled or return to active work; • The date you attain age 65; or • The expiration of the applicable COBRA Continuation Coverage period. Summary of Periods of Continuation Coverage Qualifying Event Resulting i n Loss of Coverage Qualified Beneficiary Maximum Continuation Coverage Period 1. Termination of participant (for reasons other than gross misconduct Employee, Spouse, and Dependent Children 24 months after the date of the qualifying event 1 2. Participant reduction in work hours (making the participant ineligible for the coverage in place prior to reduction) Employee, Spouse, and covered Dependents 24 months after the date of the qualifying event 1 3. Death of Employee Surviving Spouse and Eligib le Dependent Children 36 months after the date of the qualifying event 4. Divorce or legal separation of participant Spouse or Dependent Children 36 months after the date of the qualifying event 5. Dependent child ceases to qualify for benefits under the Plan Child aging out of eligibility 36 months after the date of the qualifying event
 2018 BTF Plan C Page 24 Page 26
2018 BTF Plan C Page 24 Page 26