
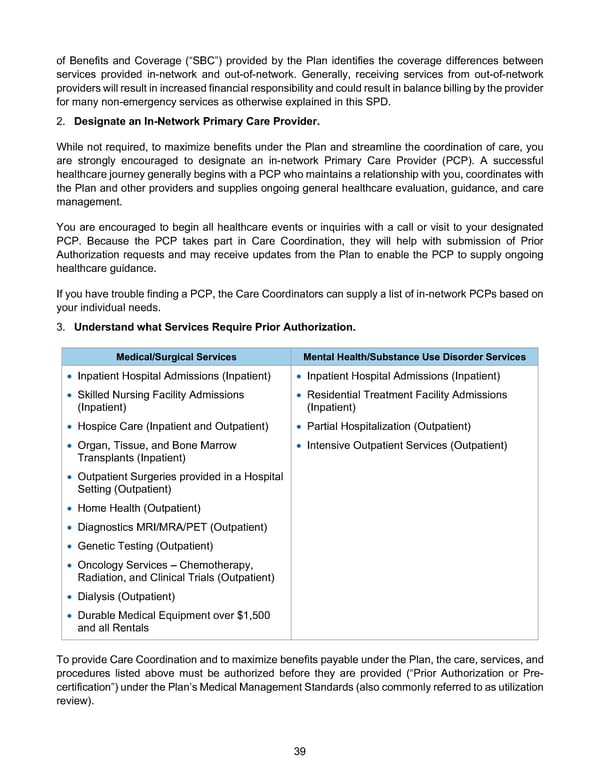
39 of Benefits and Coverage (“SBC”) provided by the Plan identifies the coverage differences between services provided in-network and out-of-network. Generally, receiving services from out-of-network providers will result in increased financial responsibility and could result in balance billing by the provider for many non-emergency services as otherwise explained in this SPD. 2. Designate an In-Network Primary Care Provider. While not required, to maximize benefits under the Plan and streamline the coordination of care, you are strongly encouraged to designate an in-network Primary Care Provider (PCP). A successful healthcare journey generally begins with a PCP who maintains a relationship with you, coordinates with the Plan and other providers and supplies ongoing general healthcare evaluation, guidance, and care management. You are encouraged to begin all healthcare events or inquiries with a call or visit to your designated PCP. Because the PCP takes part in Care Coordination, they will help with submission of Prior Authorization requests and may receive updates from the Plan to enable the PCP to supply ongoing healthcare guidance. If you have trouble finding a PCP, the Care Coordinators can supply a list of in-network PCPs based on your individual needs. 3. Understand what Services Require Prior Authorization. To provide Care Coordination and to maximize benefits payable under the Plan, the care, services, and procedures listed above must be authorized before they are provided (“Prior Authorization or Pre- certification”) under the Plan’s Medical Management Standards (also commonly referred to as utilization review). Medical/Surgical Services Mental Health/Substance Use Disorder Services • Inpatient Hospital Admissions (Inpatient) • Skilled Nursing Facility Admissions (Inpatient) • Hospice Care (Inpatient and Outpatient) • Organ, Tissue, and Bone Marrow Transplants (Inpatient) • Outpatient Surgeries provided in a Hospital Setting (Outpatient) • Home Health (Outpatient) • Diagnostics MRI/MRA/PET (Outpatient) • Genetic Testing (Outpatient) • Oncology Services – Chemotherapy, Radiation, and Clinical Trials (Outpatient) • Dialysis (Outpatient) • Durable Medical Equipment over $1,500 and all Rentals • Inpatient Hospital Admissions (Inpatient) • Residential Treatment Facility Admissions (Inpatient) • Partial Hospitalization (Outpatient) • Intensive Outpatient Services (Outpatient)
 BTF Summary Plan A/A+ Page 43 Page 45
BTF Summary Plan A/A+ Page 43 Page 45