
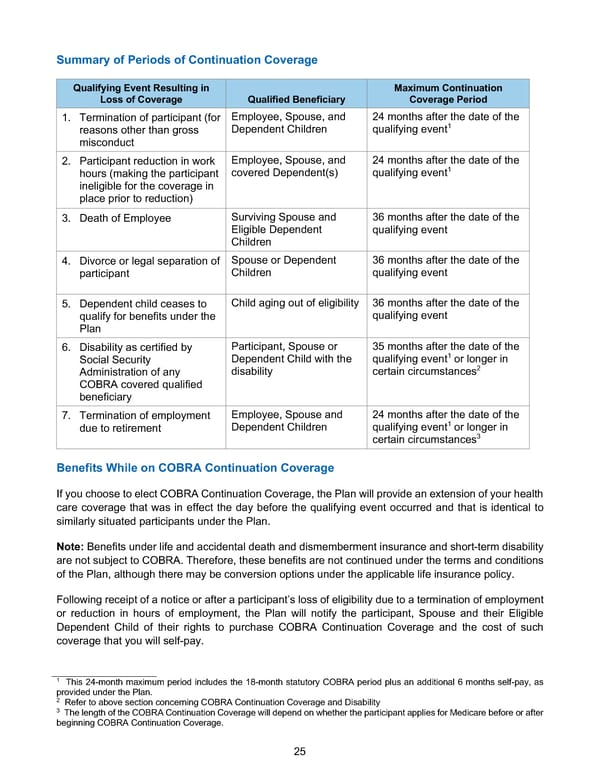
25 Summary of Periods of Continuation Coverage Qualifying Event Resulting in Loss of Coverage Qualified Beneficiary Maximum Continuation Coverage Period 1. Termination of participant (for reasons other than gross misconduct Employee, Spouse, and Dependent Children 24 months after the date of the qualifying event1 2. Participant reduction in work hours (making the participant ineligible for the coverage in place prior to reduction) Employee, Spouse, and covered Dependent(s) 24 months after the date of the qualifying event1 3. Death of Employee Surviving Spouse and Eligible Dependent Children 36 months after the date of the qualifying event 4. Divorce or legal separation of participant Spouse or Dependent Children 36 months after the date of the qualifying event 5. Dependent child ceases to qualify for benefits under the Plan Child aging out of eligibility 36 months after the date of the qualifying event 6. Disability as certified by Social Security Administration of any COBRA covered qualified beneficiary Participant, Spouse or Dependent Child with the disability 35 months after the date of the qualifying event1 or longer in certain circumstances2 7. Termination of employment due to retirement Employee, Spouse and Dependent Children 24 months after the date of the qualifying event1 or longer in certain circumstances3 Benefits While on COBRA Continuation Coverage If you choose to elect COBRA Continuation Coverage, the Plan will provide an extension of your health care coverage that was in effect the day before the qualifying event occurred and that is identical to similarly situated participants under the Plan. Note: Benefits under life and accidental death and dismemberment insurance and short-term disability are not subject to COBRA. Therefore, these benefits are not continued under the terms and conditions of the Plan, although there may be conversion options under the applicable life insurance policy. Following receipt of a notice or after a participant’s loss of eligibility due to a termination of employment or reduction in hours of employment, the Plan will notify the participant, Spouse and their Eligible Dependent Child of their rights to purchase COBRA Continuation Coverage and the cost of such coverage that you will self-pay. 1 This 24-month maximum period includes the 18-month statutory COBRA period plus an additional 6 months self-pay, as provided under the Plan. 2 Refer to above section concerning COBRA Continuation Coverage and Disability 3 The length of the COBRA Continuation Coverage will depend on whether the participant applies for Medicare before or after beginning COBRA Continuation Coverage.
 BTF Summary Plan A/A+ Page 29 Page 31
BTF Summary Plan A/A+ Page 29 Page 31