
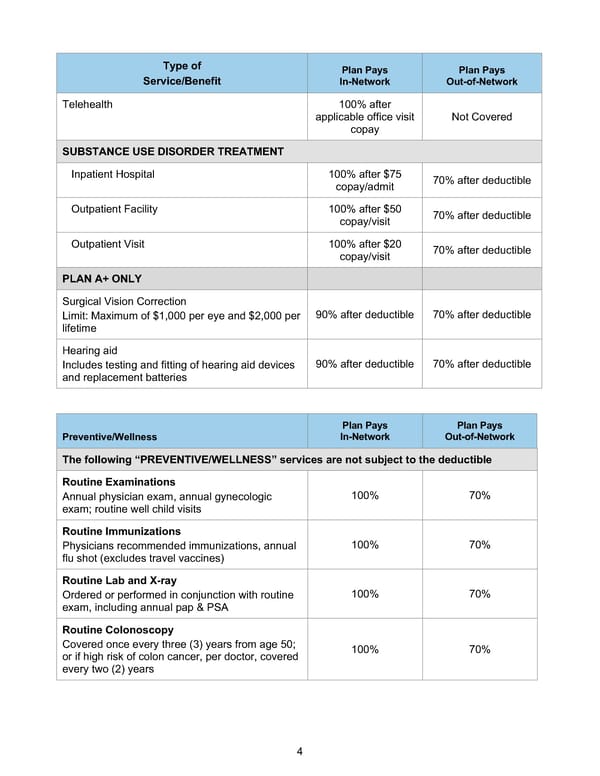
4 Type of Service/Benefit Plan Pays In-Network Plan Pays Out-of-Network Telehealth 100% after applicable office visit copay Not Covered SUBSTANCE USE DISORDER TREATMENT Inpatient Hospital 100% after $75 copay/admit 70% after deductible Outpatient Facility 100% after $50 copay/visit 70% after deductible Outpatient Visit 100% after $20 copay/visit 70% after deductible PLAN A+ ONLY Surgical Vision Correction Limit: Maximum of $1,000 per eye and $2,000 per lifetime 90% after deductible 70% after deductible Hearing aid Includes testing and fitting of hearing aid devices and replacement batteries 90% after deductible 70% after deductible Preventive/Wellness Plan Pays In-Network Plan Pays Out-of-Network The following “PREVENTIVE/WELLNESS” services are not subject to the deductible Routine Examinations Annual physician exam, annual gynecologic exam; routine well child visits 100% 70% Routine Immunizations Physicians recommended immunizations, annual flu shot (excludes travel vaccines) 100% 70% Routine Lab and X-ray Ordered or performed in conjunction with routine exam, including annual pap & PSA 100% 70% Routine Colonoscopy Covered once every three (3) years from age 50; or if high risk of colon cancer, per doctor, covered every two (2) years 100% 70%
 BTF Summary Plan A/A+ Page 8 Page 10
BTF Summary Plan A/A+ Page 8 Page 10