
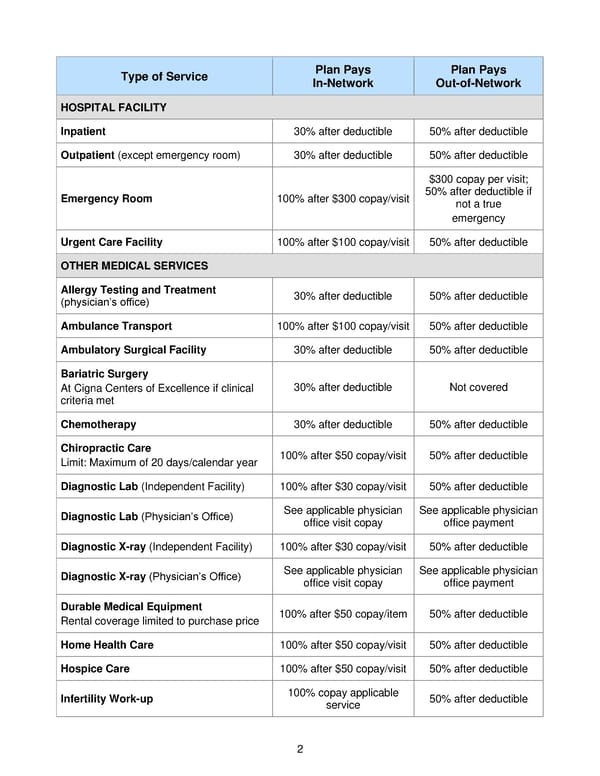
2 Type of Service Plan Pays In - Network Plan Pays Out - of - Network HOSPITAL FACILITY Inpatient 30 % after deductible 50% after deductible Outpatient (except emergency room) 30 % after deductible 50% after deductible Emergency Room 100% after $ 300 copay /visit $300 copay per visit; 50% after deductible if not a true emergency Urgent Care Facility 100% after $ 100 copay /visit 50% after deductible OTHER MEDICAL SERVICES Allergy Testing and Treatment (physician’s office) 30% after deductible 50% after deductible Ambulance Transport 100% after $100 copay / visit 50% after deductible Ambulatory Surgical Facility 30 % after deductible 50% after deductible Bariatric Surgery At Cigna Centers of Excellence if clinical criteria met 30% after deductible Not covered Chemotherapy 30 % after deductible 50% after deductible Chiropractic Care Limit: Maximum of 20 days / calendar year 100% after $ 50 copay /visit 50% after deductible Diagnostic Lab (Independent Facility) 100% after $ 30 copay /visit 50% after deductible Diagnostic Lab (Physician’s Office) See applicable physician office visit copay See applicable physician office payment Diagnostic X - ray (Independent Facility) 100% after $ 30 copay /visit 50% after deductible Diagnostic X - ray (Physician’s Office) See applicable physician office visit copay See applicable physician office payment Durable Medical Equipment Rental coverage limited to purchase price 100% after $50 copay / item 50% after deductible Home Health Care 100% after $50 copay /visit 50% after deductible Hospice Care 100% after $ 50 copay /visit 50% after deductible Infertility Work - up 100% copay applicable service 50% after deductible
 2021 BTF Plan D2 Page 6 Page 8
2021 BTF Plan D2 Page 6 Page 8