
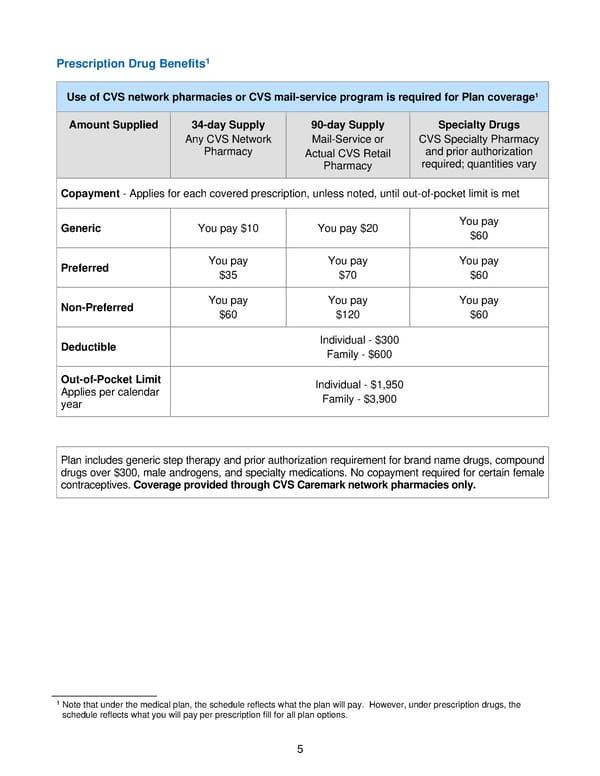
5 Prescription Drug Benefits 1 1 Note that under the medical plan, the schedule reflects what the plan will pay. However, under prescription drugs, the schedule reflects what you will pay per prescription fill for all plan options. Use of CVS network pharmacies or CVS mail - service program is required for Plan coverage 1 Amount Supplied 34 - day Supply Any CVS Network Pharmacy 90 - day Supply Mail - Service or Actual CVS Retail Pharmacy Specialty Drugs CVS Specialty Pharmacy and prior authorization required; quantities vary Copayment - Applies for each covered prescription, unless noted, until out - of - pocket limit is met Generic You pay $10 You pay $20 You pay $60 Preferred You pay $35 You pay $70 You pay $60 Non - Preferred You pay $60 You pay $120 You pay $60 Deductible Individual - $300 Family - $600 Out - of - Pocket Limit Applies per calendar year Individual - $1,950 Family - $3,900 Plan includes generic step therapy and prior authorization requirement for brand name drugs, compound drugs over $300, male androgens, and specialty medications. No copayment required for certain female contraceptives. Coverage provided through CVS Caremar k network pharmacies only.
 2021 BTF Plan D2 Page 9 Page 11
2021 BTF Plan D2 Page 9 Page 11