
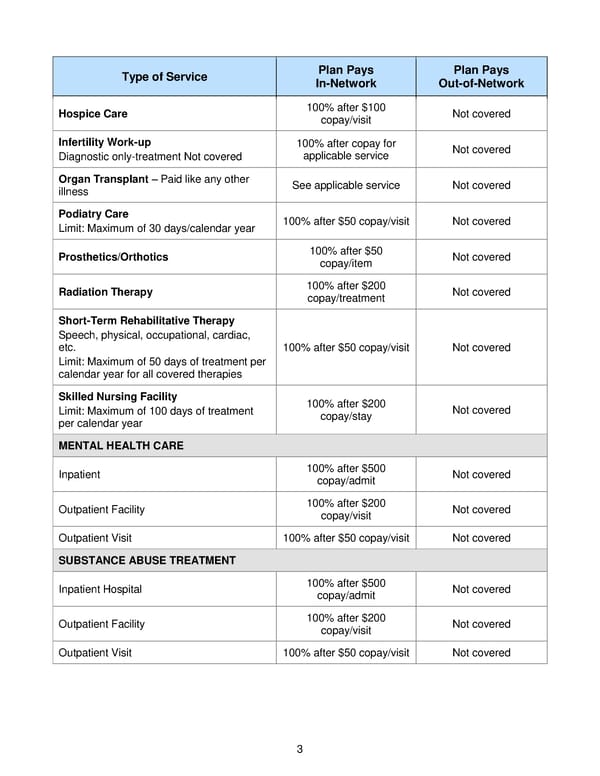
3 Type of Service Plan Pays In - Network Plan Pays Out - of - Network Hospice Care 100% after $100 copay / v isit Not covered Infertility Work - up Diagnostic only - treatment Not covered 100% after copay for applicable service Not covered Organ Transplant – Paid like any other illness See applicable service Not covered Podiatry Care Limit: Maximum of 30 days/calendar year 100% after $50 copay /visit Not covered Prosthetics/Orthotics 100% after $50 copay /item Not covered Radiation Therapy 100% after $200 copay/treatment Not covered Short - Term Rehabilitative Therapy Speech, physical, occupational, cardiac, etc. Limit: Maximum of 50 days of treatment per calendar year for all covered therapies 100% after $50 copay /visit Not covered Skilled Nursing Facility Limit: Maximum of 100 days of treatment per calendar year 100% after $200 copay / stay Not covered MENTAL HEALTH CARE Inpatient 100% after $500 copay/admit Not covered Outpatient Facility 100% after $200 copay/visit Not covered Outpatient Visit 100% after $50 copay/visit Not covered SUBSTANCE ABUSE TREATMENT Inpatient Hospital 100% after $500 copay /admit Not covered Outpatient Facility 100% after $200 copay /visit Not covered Outpatient Visit 100% after $50 copay /visit Not covered
 2018 BTF Plan C Page 7 Page 9
2018 BTF Plan C Page 7 Page 9