
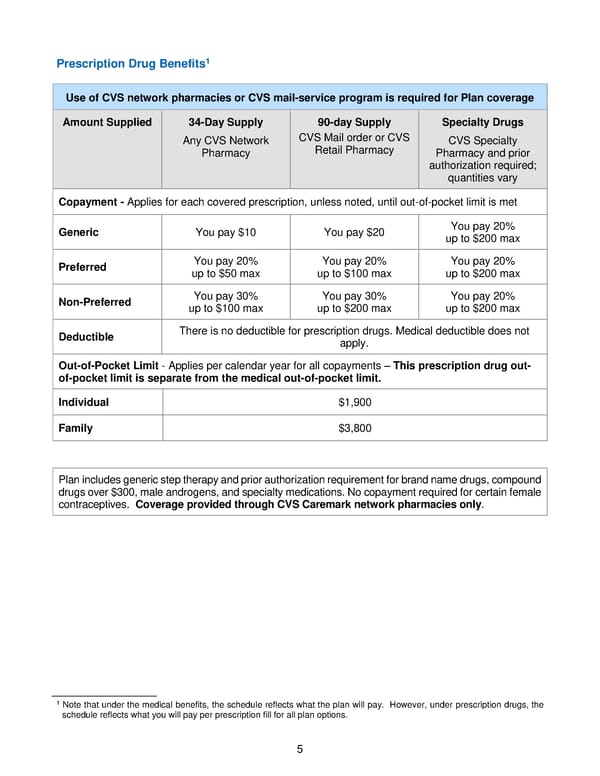
5 Prescription Drug Benefit s 1 Use of CVS network pharmacies or CVS mail - service program is required for Plan coverage Amount Suppl ied 34 - D ay S upply Any CVS Network Pharmacy 90 - day Supply CVS Mail order or CVS Retail Pharmacy Specialty Drugs CVS S pecialty P harmacy and pr ior authorization required; quantities vary Copayment - Applies for each covered prescription, unless noted, until out - of - pocket limit is met Generic You pay $10 You pay $20 You pay 20% up to $200 max Preferred You pay 20% up to $50 max You pay 20% up to $100 max You pay 20% up to $200 max Non - Preferred You pay 30% up to $100 max You pay 30% up to $200 max You pay 20% up to $200 max Deductible There is no deductible for prescription drugs. M edical deductible does not apply . Out - of - Pocket Limit - Applies per calendar year for all copayments – This prescription drug out - of - pocket limit is separate from the medical out - of - pocket limit . Individual $1,900 Family $3,800 Plan includes generic step therapy and prior authorization requirement for brand name drugs, compound drugs over $300, male androgens, and specialty medications. No copayment required for certain female contraceptives. Coverage provided through CVS Carema rk network pharmacies only . 1 N ote that under the medical benefits , the schedule reflects what the plan will pay. However, under prescription drug s , the schedule reflects what you will pay per prescription fill for all plan options.
 2018 BTF Plan C Page 9 Page 11
2018 BTF Plan C Page 9 Page 11