
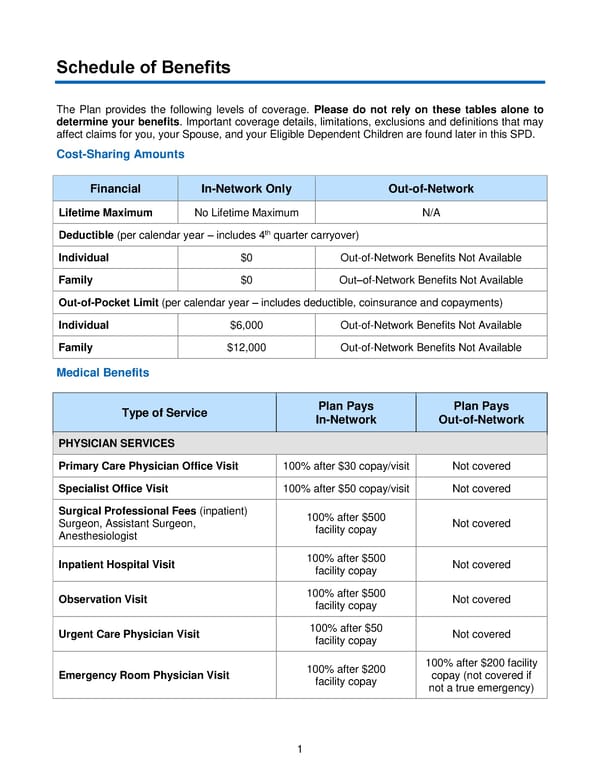
1 Schedule of Benefits The Plan provides the following levels of coverage. Please do not rely on these tables alone to determine your benefits . Important coverage details, limitations, exclusions and definitions that may affect claims for you, your Spouse, and your Eligible Dependent Children are found later in this SPD. Cost - Sharing Amounts Medical Benefits Type of Service Plan Pays In - Network Plan Pays Out - of - Network PHYSICIAN SERVICES Primary Care Physician Office Visit 100% after $30 c opay /visit Not covered Specialist Office Visit 100% after $50 copay /visit Not covered Surgical Professional Fees (inpatient) Surgeon, Assistant Surgeon, Anesthesiologist 100% after $500 facility copay Not covered Inpatient Hospital Visit 100% after $500 facility copay Not covered Observation Visit 100% after $500 facility copay Not covered Urgent Care Physician Visit 100% after $50 facility copay Not covered Emergency Room Physician Visit 100% after $200 facility copay 100% after $200 facility copay ( not covered if not a true emergency) Financial In - Network Only Ou t - of - Network Lifetime Maximum No Lifetime Maximum N/A Deductible (per calendar year – includes 4 th quarter carryover) Individual $0 Out - of - Network Benefits Not Available Family $0 Out – of - Network Benefits Not Available Out - of - Pocket Limit (per calendar year – includes deductible, coinsurance and copayments) Individual $6,000 Out - of - Network Benefits Not Available Family $12,000 Out - of - Network Benefits Not Available
 2018 BTF Plan C Page 5 Page 7
2018 BTF Plan C Page 5 Page 7